Image

Opinion | Iko Knyphausen | June 25th, 2026
Alyssa, a patient with leukemia, had exhausted all conventional treatment options. The disease persisted despite chemotherapy and a bone marrow transplant. After all standard interventions failed, her prognosis was reduced to a matter of weeks. A team at Great Ormond Street Hospital in London then proposed an unprecedented approach: they would modify three distinct genes in healthy donor immune cells without breaking any chromosomes and infuse these engineered cells into her bloodstream. The modified cells targeted and eliminated the cancer, resulting in Alyssa’s remission and discharge from the hospital.
This intervention was not a speculative or distant experimental technology. It occurred in 2022, in a clinical setting, and was made possible by a decade of transformative advances in molecular biology.
Historically, medical treatment focused on managing symptoms rather than addressing underlying causes. Missing proteins were replaced, toxins were filtered, and cancerous cells were targeted with cytotoxic agents, often with significant collateral damage to the patient. These interventions addressed the consequences of biological errors, not the errors themselves. The underlying source—the four-letter genetic code in DNA—was long considered inaccessible to direct intervention. This is no longer the case. The advent of genetic medicine has enabled the identification, targeting, and correction of errors within the human genome. Alyssa’s recovery was achieved not through conventional pharmacology but through the application of advanced molecular editing technologies.
However, the rapid advancement of genetic technologies is surpassing the capacity of existing regulatory, legal, and market institutions to govern their use. This disparity between scientific capability and institutional oversight represents a significant policy challenge.
Part I: The Molecular Toolkit
Understanding the current capabilities and implications of genetic medicine requires familiarity with the underlying molecular technologies. Over the past decade, these tools have progressed through three major developmental stages, each offering greater precision and efficacy.
The First Generation: CRISPR-Cas9
DNA is a physical macromolecule. Two long strands twist into a double helix, held together by hydrogen bonds between complementary base pairs: Adenine (A) pairs with Thymine (T), and Cytosine (C) pairs with Guanine (G). Editing this structure requires a machine that can navigate three billion letters, locate a specific sequence, and alter the chemistry at that exact coordinate.
The current workhorse of genetic medicine is CRISPR-Cas9, derived from an ancient bacterial antiviral defense mechanism. It operates on two components. The first is a guide RNA: a short molecule whose sequence is designed to match a specific target in the genome. The second is Cas9, a large protein enzyme that travels with the guide RNA and, upon arrival at the target, performs a highly energetic chemical reaction: it cleaves the phosphodiester backbone of both strands of the double helix simultaneously. This is a double-strand break. The CRISPR tool itself does not fix the gene. It severs the chromosome and walks away.1 The cell’s emergency repair machinery rushes in to rejoin the broken ends, but because this process is hasty, it frequently drops or inserts random chemical letters. The result is a disorderly genetic scar that permanently deactivates the target gene. If the clinical goal is to destroy a malfunctioning gene, this blunt instrument is devastatingly effective. If the goal is precision correction, it is poorly suited to the task.
The Second Generation: Base Editing
In 2016, a new architecture emerged that abandoned the double-strand break entirely. Base editors took the classic Cas9 protein and deliberately deactivated its scissors, rendering it incapable of cutting DNA. This modified protein, known as Cas9n (for nickase), became a programmable delivery vehicle. Chemically fused to its front end is a second enzyme: a deaminase. When deployed into a cell, the guide RNA directs Cas9n to the target site, where it unzips the double helix just enough to expose a single strand. The deaminase then performs a precise, localized chemical reaction on that exposed strand, converting a specific base, for instance, changing a Cytosine (C) into a Uracil (U), which the cell reads as a Thymine (T). To ensure this edit is permanently incorporated into both strands rather than repaired back to the original, Cas9n nicks the opposite, unedited strand. That nick signals the cell’s repair machinery to treat the edited strand as the authoritative template and reconstruct its complement accordingly. The result is a controlled, permanent single-letter substitution accomplished without triggering the cell’s emergency alarms or leaving structural scars on the chromosome.
Base editing behaves like a microscopic chemical eraser and pencil, and its clinical implications are staggering. Of the roughly 50,000 known hereditary diseases, approximately half are caused by a single-nucleotide mismatch, exactly the class of error base editors are designed to correct.2 Standard base editors are constrained to four transition mutations, the chemical conversions their deaminase enzymes can perform: C-to-T, T-to-C, A-to-G, and G-to-A. Experimental transversion editors capable of other substitutions have been reported, but remain at an early stage.3 Base editors of any kind cannot insert new sequences or delete unwanted ones.
The Third Generation: Prime Editing
In 2019, researchers unveiled the most sophisticated genetic tool yet constructed: prime editing. If traditional CRISPR is a pair of scissors and base editing is an eraser, prime editing is a search-and-replace word processor.
A prime editor fuses the deactivated Cas9 to a reverse transcriptase enzyme, a machine capable of writing new DNA code directly from an RNA template. The primary guide tool, known as a pegRNA, does two things simultaneously: it locates the exact chromosomal coordinate and carries the replacement text, the precise sequence of healthy letters to be installed. When the prime editor arrives at its destination, the reverse transcriptase reads the pegRNA’s RNA extension and physically prints a new strand of DNA, letter by letter, directly adjacent to the mutation. But the architecture requires a second actor. Physics intervenes: the longer the replacement sequence, the greater the spatial distance between the two strands of the helix at that location, placing the opposing strand out of reach for a single docked molecule. A second guide RNA is therefore dispatched to find the same chromosomal position on the opposite strand, where it nicks that strand at a calculated offset. This nick signals the cell’s repair machinery to incorporate the newly printed strand as the authoritative sequence and rebuild the opposing strand from it. Prime editing can perform all twelve possible single-base substitutions, including the transversion mutations that standard base editors cannot perform, and can also insert new sequences or delete unwanted ones, all without requiring a double-strand break or a donor DNA template.4
Part II: The Clinical Frontlines
Given the precision plus safety advantages of base and prime editing, one might assume that modern hospitals are already widely deploying them. The reality of the clinic tells a different story.
The Regulatory Time Lag
The primary reason traditional CRISPR dominates approved therapies is chronological, not scientific. CRISPR-Cas9 was described in 2012. Therapies built on it began clinical trials nearly a decade ago. The approvals crossing the regulatory finish line today reflect the finest science of the mid-2010s. Drug development advances in an unyielding pipeline. Phase I trials test basic safety in a handful of patients. Phase II evaluates efficacy and dosing. Phase III expands to large, diverse cohorts. This process commonly takes 8 to 10 years. Base editing (2016) and prime editing (2019) are moving through that pipeline at unprecedented speed, presently navigating Phase I and Phase II trials. They have not yet achieved widespread commercial authorization because they are younger technologies, not inferior ones.
When Blunt Is Best
There is a strategic reason why traditional CRISPR remains the tool of choice in certain applications. Sometimes a blunt instrument is exactly what the clinical situation requires.
CAR-T cell therapy illustrates this precisely. Scientists extract T-cells from a patient’s immune system, take them to a laboratory, and use genetic engineering to insert a Chimeric Antigen Receptor (CAR), a molecular radar that enables the T-cell to locate and destroy cancer cells. But tumor cells are evolutionarily sophisticated. They express a protein called PD-L1 that binds to the PD-1 receptor on T cells, suppressing immune activation and allowing the cancer to evade destruction.
To make an effective CAR-T therapy, scientists must permanently inactivate the PD-1 gene in the engineered T cells. Instead of correcting a few letters, the goal is to obliterate the gene so thoroughly that the brake pad can never be manufactured again. For this specific purpose, the double-strand break is the ideal tool. The chaotic, error-prone repair scar permanently disables PD-1, allowing the engineered cell to pursue the tumor unimpeded.5 In cancer treatment, the bluntness of first-generation CRISPR is a feature.
Breakthroughs Already in Human Trials
Despite their youth, next-generation editors have already proven their capabilities in human patients. Alyssa’s treatment required three simultaneous gene edits inside donor T-cells: one to prevent them from attacking her body, one to prevent them from attacking each other, and one to render them invisible to chemotherapy drugs. Performing three separate double-strand cuts with traditional CRISPR in a single cell risks catastrophic chromosomal collapse. Base editors executed all three edits safely, without breaking the backbone of a single chromosome. The therapy cleared her cancer.6
Prime editing has now made its own historic leap from laboratory to human physiology. A pioneering clinical trial for Chronic Granulomatous Disease, a rare, life-threatening immune deficiency caused by a specific genetic mutation in blood stem cells, initiated human dosing with a prime editing therapeutic designated PM359. Early results have validated the safety profile that decades of molecular biology predicted.7
Part III: The Ethical Dimension
Science has achieved escape velocity. What has not kept pace is everything built to govern, distribute, and constrain it: the laws, the institutions, the markets, and the ethical frameworks. What follows is a map of a single, serious structural failure, the distance between what genetic medicine can now do and what civilization has arranged to handle.
The Gattaca Problem8
Germline editing, altering the DNA of a human embryo in a way that would be inherited by every subsequent generation, is broadly prohibited across the major scientific powers. The United States, the United Kingdom, and the European Union all enforce legal barriers. The International Commission on the Clinical Use of Human Germline Genome Editing, convened jointly by the National Academies of Sciences and the Royal Society, concluded in 2020 that heritable human genome editing should not proceed until robust oversight mechanisms are in place.9
But prohibition is not prevention. In November 2018, He Jiankui, a Chinese biophysicist trained partly at Rice University, announced the birth of twin girls whose embryos he had edited using CRISPR-Cas9 to disable the CCR5 gene, attempting to confer resistance to HIV. He was subsequently tried, convicted of illegal medical practice, and sentenced to three years in prison.10 The twins, now school-age children, carry permanent genomic modifications in every cell of their bodies. So will their children. He operated in a jurisdiction that had guidelines but, at the time, no hard statutory prohibition. Multiple other countries have no legislation governing germline editing whatsoever. As CRISPR equipment becomes cheaper and more widely available, consumer-grade bacterial genome-engineering kits are already sold online for under $200,11 and the pressure on the perimeter of existing prohibitions will grow. The law that stopped He Jiankui was the Chinese criminal law applied ex post facto. There is no international enforcement mechanism, no treaty body with authority to investigate, and no agreed-upon standard for what constitutes an acceptable versus unacceptable edit.
The Gattaca problem is not hypothetical. It is already documented, already embodied in two living children, and already expanding toward an unmonitored global market.
The Weapons Problem
DARPA, the Defense Advanced Research Projects Agency, has invested substantially in genetic biodefense research. Its Safe Genes program, launched in 2017, funds the development of tools to counter potential genetic threats, including gene drives, engineered sequences capable of propagating through an entire wild population within a few generations.12 The program is explicitly defensive in framing. The underlying technology is not inherently so.
The Biological Weapons Convention of 1972 prohibits the development, production, and stockpiling of biological weapons. It was negotiated when the most sophisticated genetic manipulation available was selective breeding. Crucially, it has no verification protocol, no inspection regime, and no enforcement body with meaningful authority. Nations sign it and are taken at their word. Nine review conferences have been held since 1972, most recently in 2022; none has produced a binding verification mechanism.13
Base editing and prime editing can, in principle, be applied to pathogens as readily as to patients. A base editor targeted at a bacterial chromosome could silence the genes that make the antibiotic effective against it. A prime editor could insert sequences into a viral genome with a specificity that natural mutation cannot approach. This is not conjecture. The mechanistic capability is the same technology reviewed in Part I, redirected at a different target organism.
The Geneva Protocol, which first prohibited biological weapons, dates to 1925. Science has advanced by several orders of magnitude in the intervening century. The treaty architecture has not kept pace.
The Patent Problem
The core intellectual property dispute over CRISPR is one of the most consequential and least publicly understood legal conflicts in modern science. The Broad Institute, representing MIT and Harvard, and the University of California, Berkeley, have spent years and hundreds of millions of dollars litigating who owns the core patents on CRISPR-Cas9 technology in eukaryotic cells, the cells of which all animals, including humans, are made.14
The practical consequence is that whoever holds controlling patents determines who can commercialize life-saving therapies, under what licensing terms, and at what price. A university spin-out attempting to develop a CRISPR-based cure for a rare disease must first navigate a patent estate whose ownership has been contested in federal court for a decade.
Base editing and prime editing each have their own patent estates, developed substantially at the Broad Institute by biochemist David Liu. They are not automatically resolved by the CRISPR-Cas9 litigation outcome. But they are not immune to downstream licensing complications when delivery vehicles, guide RNA designs, and cellular application methods overlap with contested foundational claims. The field has responded by establishing a web of cross-licensing arrangements. Those arrangements are negotiated between well-capitalized institutions. An independent researcher or a small biotech in a developing country has no seat at that table.
We have placed the keystone of a public health revolution within a patent thicket whose primary beneficiaries are law firms and technology transfer offices at elite American universities.
The Access Problem
In December 2023, the FDA approved Casgevy, a CRISPR-based therapy for sickle cell disease and transfusion-dependent beta-thalassemia, developed by Vertex Pharmaceuticals and CRISPR Therapeutics. It is the first approved CRISPR therapy in the United States. Its list price is $2.2 million per patient.15
Sickle cell disease affects approximately 100,000 Americans. Roughly 90 percent of them are Black.16 The therapy that can functionally cure the disease they disproportionately carry is priced at roughly eighteen times the median American household net worth of $121,700, as reported in the Federal Reserve’s 2022 Survey of Consumer Finances.17
Medicare and Medicaid reimbursement frameworks were designed for recurring pharmaceutical costs: monthly prescriptions, annual infusions, and ongoing treatment protocols. A one-time curative therapy that eliminates all future disease costs over a patient’s lifetime does not cleanly fit that model. Insurers face an actuarial disincentive: they may pay the full $2.2 million for a cure only to have the patient switch plans, with the long-term savings accruing to a competitor. The Institute for Clinical and Economic Review has noted this misalignment explicitly in its analyses of gene therapy financing.18
The result is a system in which a genetic cure exists, is approved, and remains practically inaccessible to the majority of the population it was designed to serve. It is a predictable structural consequence of applying twentieth-century insurance architecture to twenty-first-century medicine.
Part IV: The Regulatory Vacuum
Underlying all four of the above failures is a single institutional problem: the regulatory framework governing genetic medicine was built for a technology that no longer exists.
The FDA’s gene therapy oversight architecture was constructed in the 1990s, following the 1999 death of Jesse Gelsinger, an eighteen-year-old who died during a gene therapy trial at the University of Pennsylvania from a massive immune reaction to the viral delivery vehicle.19 That framework was designed around viral vectors, disabled viruses used to ferry corrective genes into cells. It was not designed for molecular machines that change individual chemical letters without breaking chromosomal backbones.
Base editing and prime editing are being evaluated under regulatory frameworks that treat them as variants of viral gene therapy, because no alternative classification yet exists. Epigenetic editing, which attaches or removes chemical tags that control whether genes are expressed without altering any DNA letters, may not qualify as gene therapy under current FDA definitions. If that classification gap holds, it could advance through clinical development in a regulatory category for which the risk assessment protocols are entirely mismatched to the actual mechanism of action.
The delivery platform compounds this. Lipid nanoparticles, the tiny engineered fat bubbles that carry mRNA or gene editing machinery into cells, were validated at an unprecedented scale by the COVID-19 mRNA vaccine program. Hundreds of millions of people received LNP-delivered mRNA sequences. That program demonstrated, at a population level, that LNP delivery is broadly safe and feasible.20 The same platform now carries base and prime editors into liver cells in ongoing clinical trials.21
The public absorbed the proof of concept. Congress did not draw the regulatory inference. The FDA has issued guidance documents on gene therapy manufacturing and on the use of CRISPR in clinical trials, but no comprehensive statutory update to the underlying framework has been enacted. The agency is regulating third-generation molecular technology under a framework designed during the Clinton administration.22
The Verdict
Alyssa is alive. That is the undeniable achievement of this era of medicine. A tool of extraordinary power has arrived, and it works.
The landscape around that tool is ungoverned in ways that should alarm anyone paying attention. Germline editing is technically prohibited and practically unenforceable across large portions of the globe. The biological weapons treaty, supposed to prevent states from weaponizing these technologies, has been reviewed nine times without producing a single verification mechanism. The intellectual property system has placed control of the underlying science at the center of a patent dispute between two elite research universities. The insurance market cannot pay for cures that work the first time. And the regulatory agency charged with overseeing it is operating under a framework established during the Clinton administration.
Science has written the future. The institutions supposed to shape how that future arrives are not keeping pace.
Closing that gap does not require slowing the research. It requires building institutions fast enough to deserve the science.
The author can be reached via email at iko@uw.edu
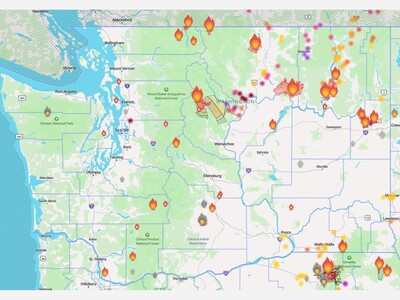
Smoky haze, with a high of 87 and low of 54 degrees. Smoky haze for the morning, clear overnight.

After I completed the very first Community Police Academy (I would highly recommend participating in this), I had the honor of doing my "ride along" with Sgt Walker. A true compassionate professional and an asset to our LFP police department.

What an excellent choice. Chief Zanella will do an excellent job leading our LFP PD.